Ankle & Syndesmotic Injuries
Acute Ankle Sprains
- Acute ankle sprains are common and generally recover very well.
- Ankle sprains can occur at any age.
- Most often, the ankle rolls inwards- which is called inversion- to cause these injuries and most of the time you can take a few steps even though there is pain when putting weight on the ankle.
- A grade 1 injury is the most common and generally just involves this ligament at the front called the Anterior talofibular ligament. People generally recover very well and function even if this ligament does not heal fully.
- A grade 2 injury occurs as more force is put into that inverted position and then partially or fully tears the next ligament in the line called the CFL or calcaneofibular ligament.
- A grade 3 injury is the highest grade with full tears of both ligaments and sometimes even with injury to ligaments toward the back of the ankle.
It’s important to realise that the evidence overall does not show a correlation between the grade of injury and long term outcome.
Higher grade injuries may do better with early immobilization but only very short term- less than 10 days because this can lead to increased stiffness.
We know there is an increased risk of re-injuring the same ankle because the torn ligaments serve proprioceptive functions, and this is the main value in ensuring patients invest in a proper course of rehab- for future injury prevention.


Chronic Ankle Instability
Unfortunately, some patients progress to recurrent ankle sprains, which are frustrating and may predispose to ankle joint damage.
The reason a doctor needs to really listen to what a patient is saying here is that Instability is something that only a patient can tell us, not something that can be concluded simply by examination.
A patient who does not trust their ankle, is worried about walking in the dark and has usually had a number of sprains has chronic ankle instability. 4,7
They may also have pain between episodes and most have had to modify their lifestyle and activities around this injury.
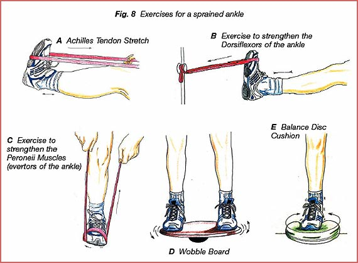
The most common cause of this is inadequate rehabilitation, and most clinicians do not refer patients without other serious problems for surgery until they have trialed good quality rehab for at least 6 weeks, in combination with bracing and taping to assist proprioception.

Evidence shows that taping and bracing reduce the risk of recurrent sprain immediately, to the same level that rehab alone would by 10 weeks.

If despite this, there is ongoing ankle pain, swelling and over 3 episodes of significant ankle sprains in a year, then a patient with chronic ankle instability really should see a foot and ankle surgeon for an opinion.
Ankle Syndesmosis Injuries
People with an external “foot out” rotational mechanism, generalized swelling and pain higher up on the ankle- this could be a syndesmosis or high ankle injury which may be unstable and should be referred for a further workup.
Most of the time, it’s very hard to remember which way the foot went so when there is pain higher than expected we need to be on alert for this potential injury.
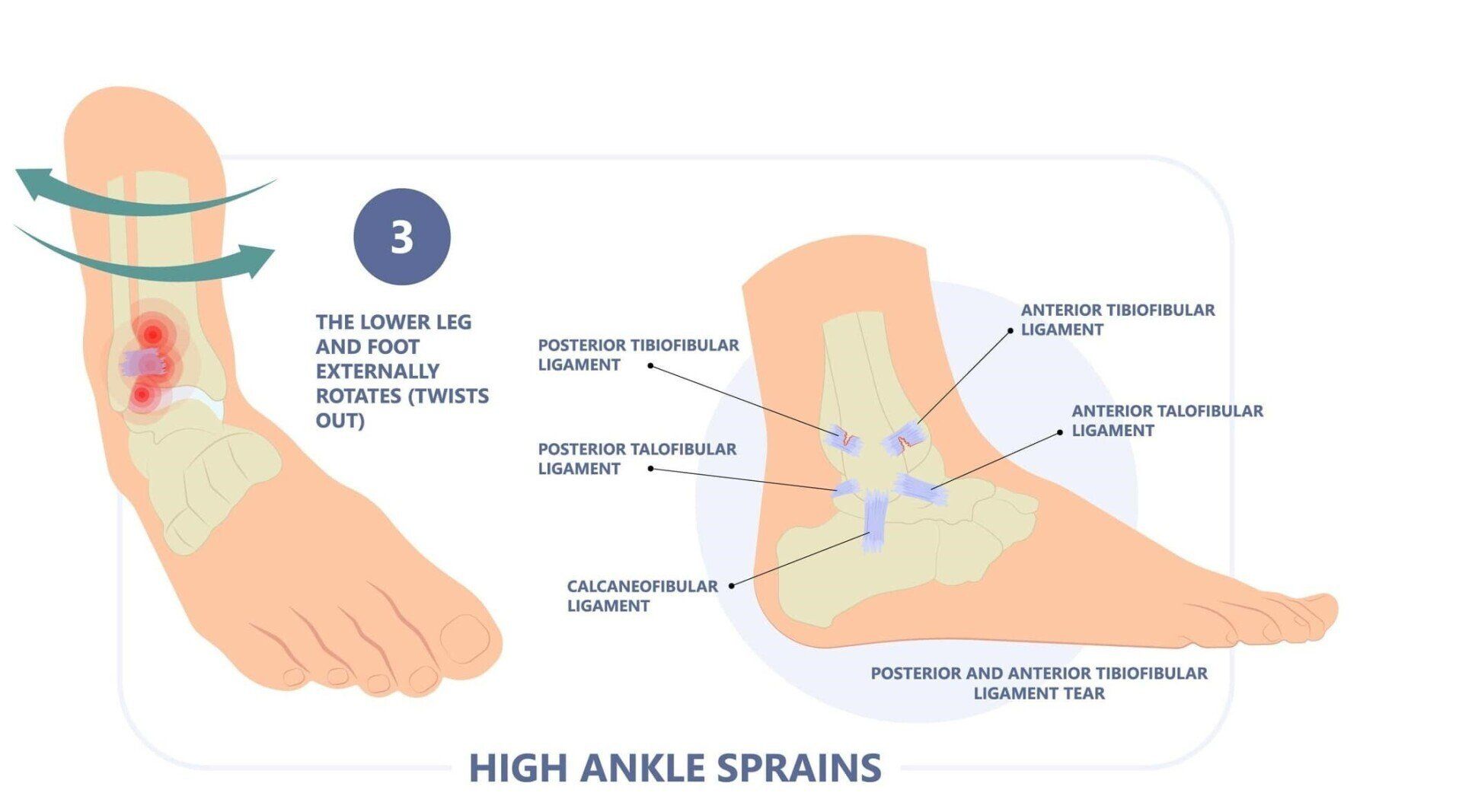

You can see in the animation in the video that the ankle joint normally functions like a hinge with the two lower bones of the leg (the tibia and fibula) locking into the saddle shaped bone in the middle called the talus.
When a forceful sideways motion occurs, this opens the hinge and spreads the strong ligaments that hold the two bones together.
It always occurs in a front to back pattern like a book opening up and therefore tenderness around this area of the ankle is quite suggestive of injury
Diagnosis & Treatment of Syndesmosis Ankle Injuries
The diagnosis can be made quite confidently through a combination of clinical tests, but An ultrasound adds the advantage of being able to see this ligament at the front for any damage.
MRI can determine whether there are any associated injuries inside the ankle joint.
As with any acute injury the principles are to control the initial inflammatory response with rest/optimal loading, ice/compression/elevation.
The severity of ligament damage or associated cartilage or bony injury determine whether surgery is needed.
Most cases are lower grade injuries that can certainly be managed non-operatively as outlined below, with the use of a stirrup that helps push the ends of the bone together to accommodate ligament healing in a tighter more functional position.
In my previous research we found that rugby players with these injuries were able to return to play an average of 3 weeks sooner with a single PRP injection to the torn ligament, in combination with standard rehabilitation.

Rehabilitation Milestones:
- Requires surgery if unstable
- Expect 6–10-week recovery if stable
- Single Platelet-rich-plasma injection may accelerate recovery
- Ankle Stirrup (or Boot) and non-weight bearing until pain-free double leg lunge
- Ankle Stirrup and walking only until pain-free single leg lunge
- Ankle Stirrup and cross training (bike, pool, Alter-G) until pain-free hopping
- Ankle Stirrup and straight line running
- Sport specific rehabilitation once pain-free running for 1 week
- Stirrup should be weaned gradually