(02) 8540 8019


Rotator Cuff (Impingement) Syndrome
Swimmer's Shoulder is a condition that covers a broad spectrum of pathology.
Due to repetitive overhead activity, there is mechanical irritation of the tissues under the arch of the shoulder and this is called
SHOULDER BURSITIS and IMPINGEMENT.
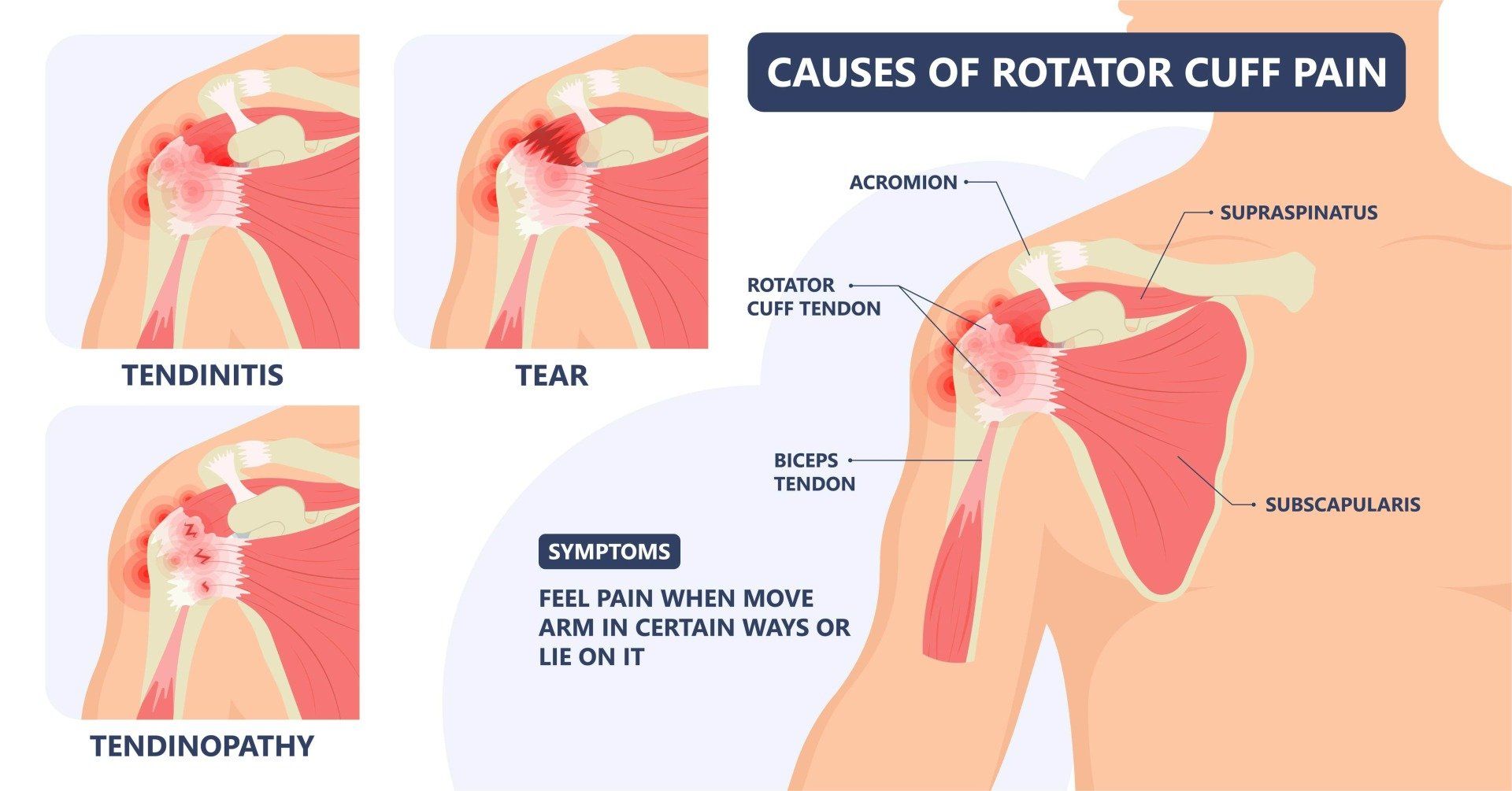
As it progresses, the rotator cuff tendon becomes irritated and then develops features of disrepair.
When microscopic tears come together over a long period of time, and as the rate of tissue breakdown slowly exceeds the rate of repair, this transitions into ROTATOR CUFF TENDINOPATHY and TEARS.
Subacromial Bursitis and Shoulder Impingement
The shoulder is a complex joint where several bones, muscles, and ligaments connect the upper extremity to the chest.
The subacromial space is the area underneath the bony arch of the shoulder, which like many areas of tissue movement, has a bursa.
A bursa is a layer of tissue that helps tissue planes glide- it is basically a thin lubricating fluid sac.
In the above video, you will see an anatomical section of the shoulder with the ball and socket, the rotator cuff and this layer of tissue is easily seen that helps it slide under the bony arch of the shoulder as you lift your arm up.
Just like most forms of deep bursitis, it often coexists with tendon irritation and wear.
When the bursa becomes inflamed it swells and causes pain.
Inflammation leads to swelling and thickening of the tendons and bursa causing space reduction that may further squeeze or compress the rotator cuff tendon and bursa itself. More importantly, pain leads to maladaptive movement of the shoulder so that imbalances in muscle forces tend to push the ball upward in the socket, again leading to pinching of the tendons under the bone. The cycle continues- and this compression results in pain, tenderness and sometimes weakness of the shoulder.
The combined condition of rotator cuff tendinosis and bursitis is called an impingement syndrome. This can be structural (due to a big spur or narrowing under the acromion) or functional (due to poor rotator cuff function and force imbalances).
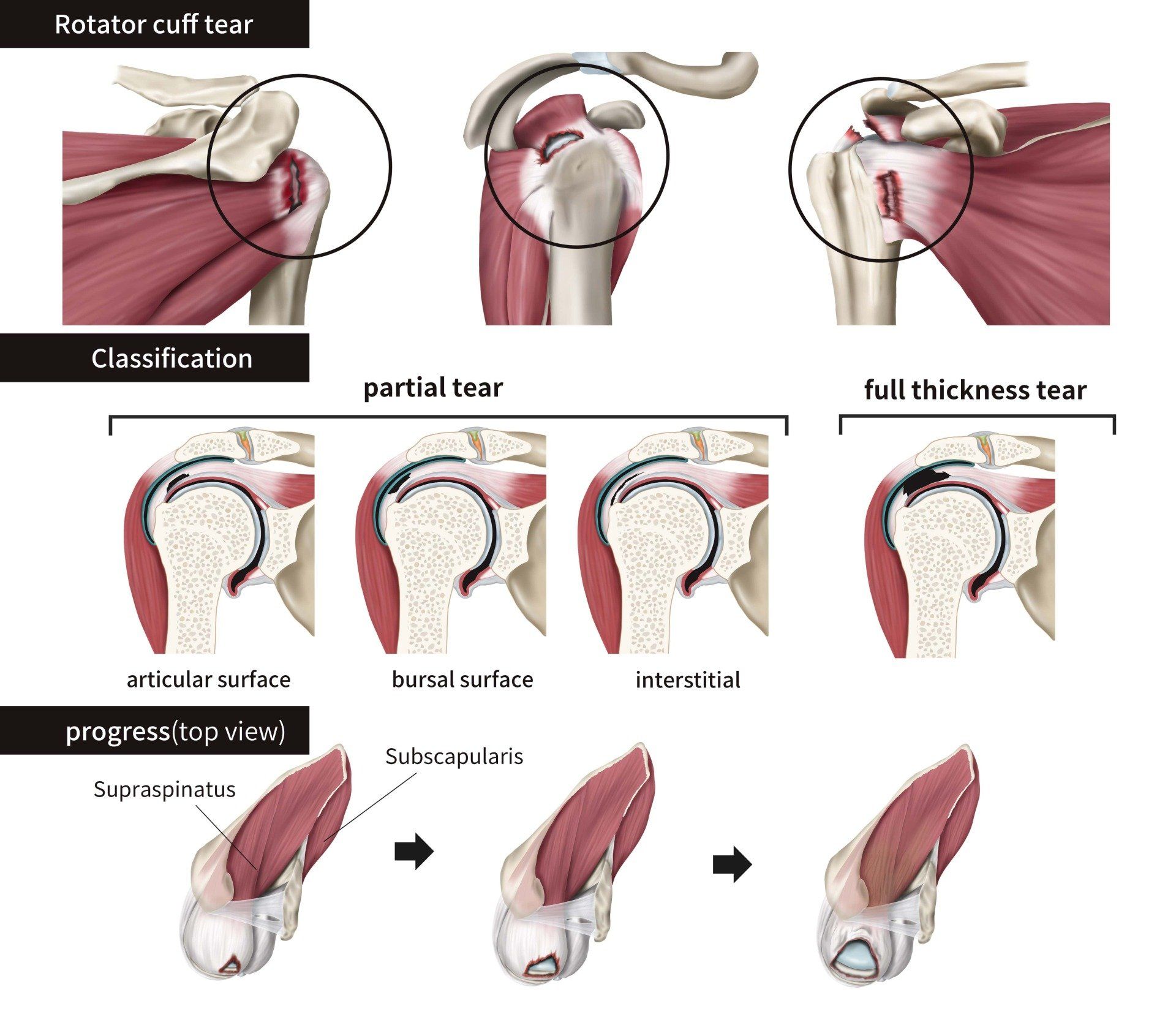
With age and with continued repetitive use, rotator cuff tears can occur. When these have happened without trauma, they are usually due to wear. Most rotator cuff tears are of the top part, called the supraspinatus tendon. The tears are usually splits in the tendon referred to as partial tears (both ends are together but frayed around the edges) rather than full-thickness tears (ends are separated). When there is a big full-thickness tear, there is usually weakness and most patients require surgery to restore their strength. However, most rotator cuff tears are partial tears that happen over time due to friction and a rate of wear that exceeds recovery speed.
Causes of Subacromial Bursitis
Swimmer’s shoulder and bursitis may be caused by repeated minor trauma such as overuse of the shoulder joint and muscles during swimming, but also other activities like overhead weights, throwing and even occupational and domestic tasks.
Despite most swimmers being very well trained,
the sheer number of repetitive cycles of swimming is the major factor.
Under fatigue, the muscles that control shoulder movement and elevation, can fail to clear the space for the rotator cuff and bursa, so that impingement occurs.
Diagnosis & Treatment of Subacromial Bursitis
The medical workup for Subacromial Bursitis involves a comprehensive history, physical examination and often includes point-of-care dynamic ultrasound to assess the movement of tissues as they glide under the acromion bone.
Bursitis is a bit like smoke to fire in most cases. The bursitis is a downstream effect of abnormal shoulder mechanics. The pain inhibits normal muscle activation and then perpetuates these abnormal mechanics and usually goes with irritation of the rotator cuff itself. Hence, this requires a holistic view of treatment.
First line treatment for bursitis should be:
- Avoidance of triggers for irritation- overhead activities, lifting and anything that triggers pain
- X-rays to exclude a primary/structural source of impingement
- NSAIDs- at anti-inflammatory, not just analgesic doses- 7-10 days of use
- Rehabilitation exercises to restore balance and centring of the humeral head and stability of the base of the shoulder
- Escalation to
corticosteroid injection, a more potent anti-inflammatory treatment, if unable to make progress

This needs to be Combined with rehabilitation exercises one week after the injection so that the pain is no longer inhibiting proper muscle activation.
The results of surgical decompression are controversial, with studies showing no long-term benefit of either open or arthroscopic debridement compared to an exercise-based approach at 2 years.
If you have shoulder pain and impingement, see a health professional with expertise to get a diagnosis and treatment plan.
Rotator Cuff Tears
The rotator cuff is a broad flat group of tendons that come from the wing bone to wrap around the ball of the shoulder, which doctors call the head of the humerus.
They pull this ball into its socket and keep it centered in the socket with all movements of the shoulder.
It also helps us elevate our arm above our head and this movement is lost when the rotator cuff is not working.
Diagnosis and Treatment of Cuff Tears
When a patient presents with a painful, weak shoulder, the diagnosis of rotator cuff tears is best confirmed with MRI in corroboration with clinical examination findings, picking up around 85% of tears. Ultrasound is useful in experienced hands and can be corroborated with examination findings immediately.
As you can see from the video below, sutures with anchors that invest the tendon back to the bony footprint are used to repair a full thickness rotator cuff tear.
Full thickness tears are any tear that goes from top to bottom through the rotator cuff.
They can be wide or small, and we also measure the degree of retraction or how far the tendon ends move away from each other.



INJURIES
CONDITIONS
REHAB PROGRAMS
