Hip & Groin Pain
Hip Impingement & Labral Tears
One cause of hip and groin pain is hip impingement with labral tears.
The labrum of the hip, known as the acetabular labrum is a biological washer that improves the congruence and stability of the joint.
There are several reasons why the labrum may develop a tear, but one of the most common reasons is the shape of the hip joint lending itself toward abrasion of the labrum.
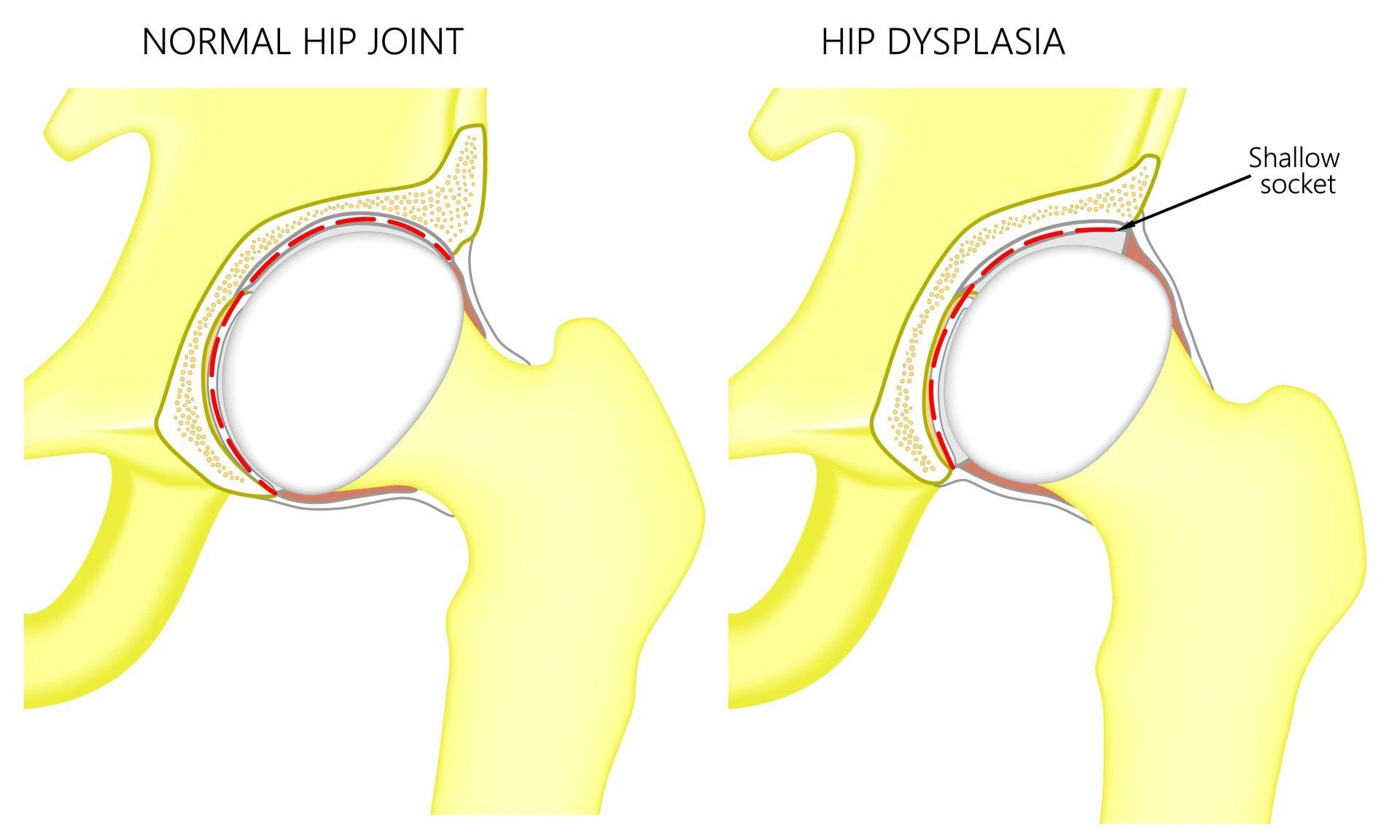
Some patients will be born with a shallower hip socket, a condition known as developmental dysplasia of the hip, and put increased load on the edge of the socket.
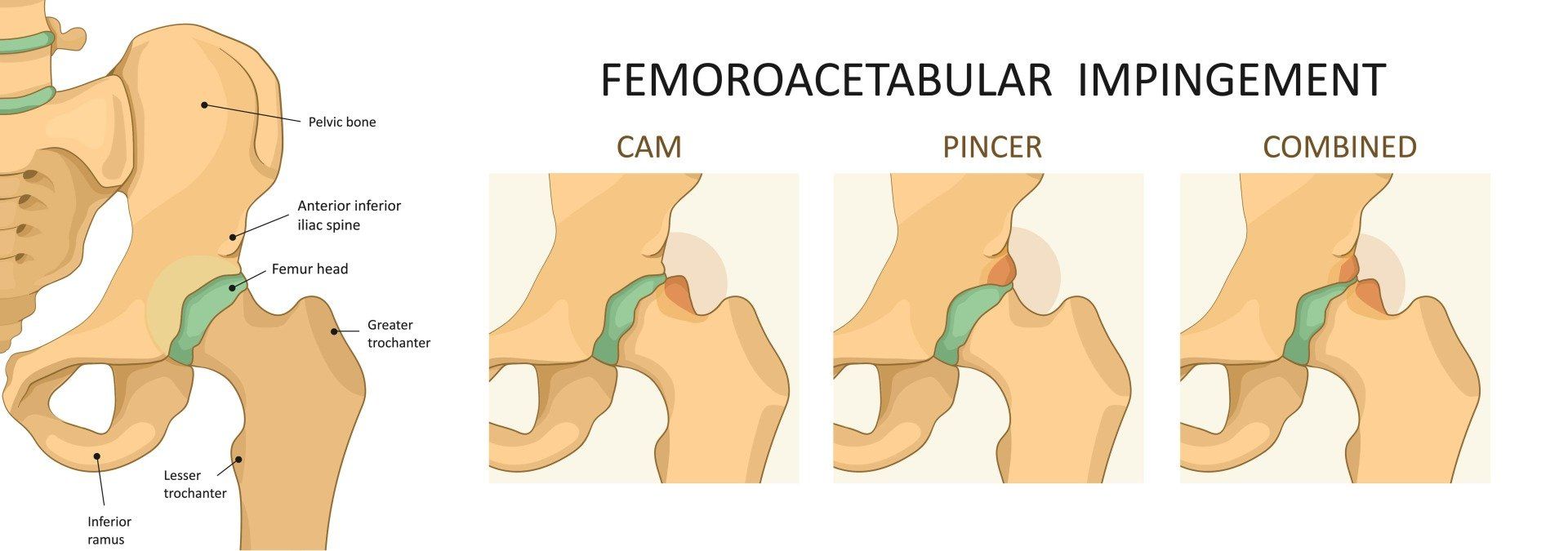
Others will develop bony bumps around their growth plates during adolescence and this leads to pinching or impingement of the soft tissues at the front of the socket, including the labrum between those bony bumps as the knee moves up toward the chest. This is called FAI or hip impingement syndrome. 1
Diagnosis of Hip and Groin Pain
One of the challenges faced by clinicians is that Tears of the labrum are not always painful. One prospective study showed that 40% of patients who had a symptomatic labral tear had completely asymptomatic tears on their other side. 2,3 As many as 55% of athletes have the criteria for FAI on scans, but only a small proportion have FAI syndrome.
Patients with symptomatic FAI syndrome often give a history of Increased squat/lunge activity or have been very Athletic across sports involving knee to chest activities like kicking sports. The pain generally is described as a deep groin pain.
On examination there is pain with reduced squat and low range in flexion (knee to chest) positions. One special test that commonly exacerbates the pain involves bringing the knee up toward the opposite shoulder and is called FADIR (Flexion ADduction Internal Rotation).

X-rays tend to show preserved joint space but a prominence around this head-neck junction and loss of the normal sphericity of the femoral head can be seen. 1
Some patients will also have a prominence of the edge of the socket, called a pincer lesion.
The labrum of the hip can only be appreciated on imaging using an MRI. An MR arthrogram is an MRI scan after the injection of contrast and this is very accurate at picking up subtle labral tears. 4
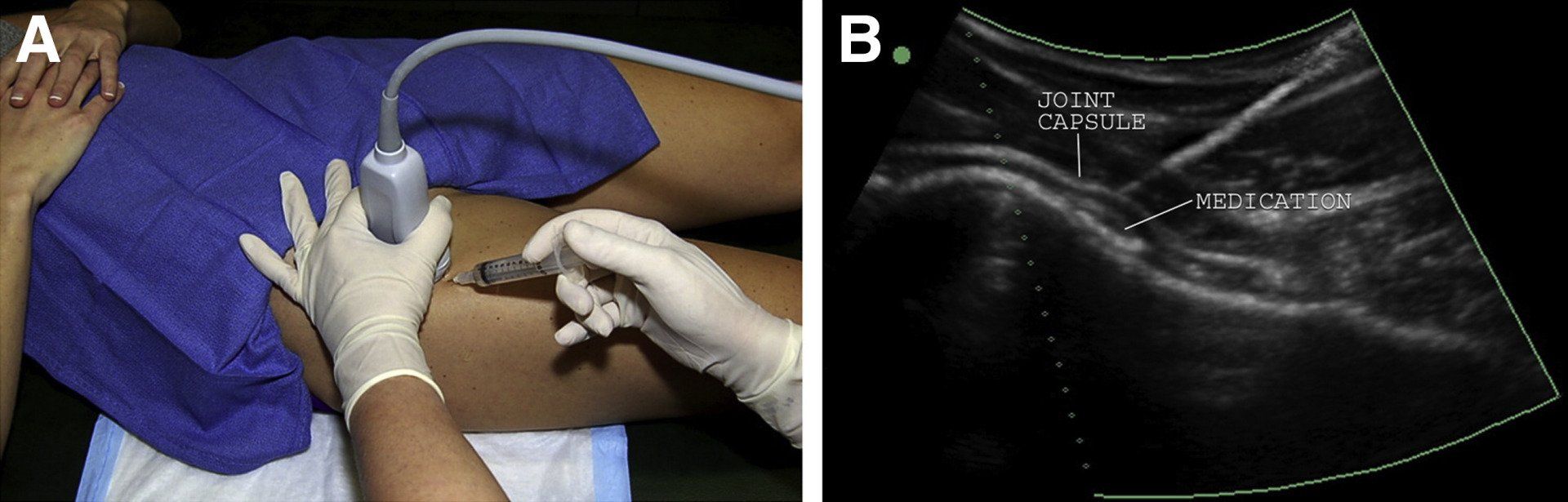
However, as I mentioned, even a tear of the labrum can be asymptomatic and so it can really help the diagnosis to undertake a local anaesthetic injection into the joint and re-test the joint in order to determine whether the pain from the labrum then goes away.
In my practice, I prefer to have patients undertake an MRI arthrogram with local anaesthetic and corticosteroid all at the same time so that we can determine if a labral tear is present, and whether that tear is causing pain.
Recommended Treatments for FAI Syndrome
Most patients with FAI syndrome and labral tears can be treated non-operatively, however it is a slow process. The Warwick consensus statement is an evidence-based guide on management of this controversial area. 6,7
The first step is to understand the biomechanics of deep squatting and lunging and how they contribute to pain and impingement, so that aggravating activities can be modified.
Patients need to understand that their hip shape or morphology has been there long-term and that there are many people with the same bone shape without any pain, and therefore changing this with surgery is not a necessary first line treatment.
When there is significant pain and the joint is quite inflamed, a course of anti-inflammatory medications or a cortisone injection for more severe symptoms can help settle the pain down to much more manageable levels. Not only can this help confirm the pain-driver is inside the hip when the local anaesthetic takes the pain away (as stated above, many patients have asymptomatic labral tears), but this can then open the door to higher quality therapeutic exercise for the stabilising muscles of the hip called the deep external rotators. A skilled rehabilitator will also address the underlying impairments of the persons movement at the lumbar spine and other joints (the so-called kinetic chain). Some patients benefit from simple proprioceptive measures like taping and orthotics.

A surgical opinion to consider hip arthroscopy is only warranted if there is significant hip deformity and severe symptoms not responding to treatment, or with a proven symptomatic labral tear after MRI and injection that hasn’t responded to a solid 4-6months of appropriate rehabilitation. 8,9
Unfortunately, patients with more severe FAI and labral tears are known to be at a higher risk of developing hip osteoarthritis in future. 6,10 However, there is no longitudinal evidence to suggest that surgery prevents hip Osteoarthritis.
Groin Pain - What are the Causes?
Groin pain is often complex and multi-factorial.
There are a
number of inter-related structures around the groin, so there is often overlap in the anatomical structures that generate pain.
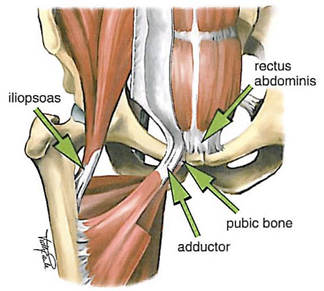
A comprehensive history and clinical examination can assist in directing the diagnosis toward the following generators of groin pain:
-Inguinal-related (inguinal hernia, sportsman’s hernia)
-Adductor-related (adductor tendinosis and tears)
-Psoas (hip flexor) related (iliopsoas tendinosis and bursitis)
-Pubic-related (pubic bone edema, pubic symphysitis)
Further advanced imaging may include pelvic X-rays (with Flamingo Views for stability), Ultrasound and MRI.
Sometimes these pain-generators in the groin coexist in the same patient. While every individual is different, it is now thought that excessive torsional and shear forces, particularly under fatigue, leads to micro-movement in the pelvis. This then leads to overload of the inguinal/ adductor and pubic structures to differing degrees (often in that order).
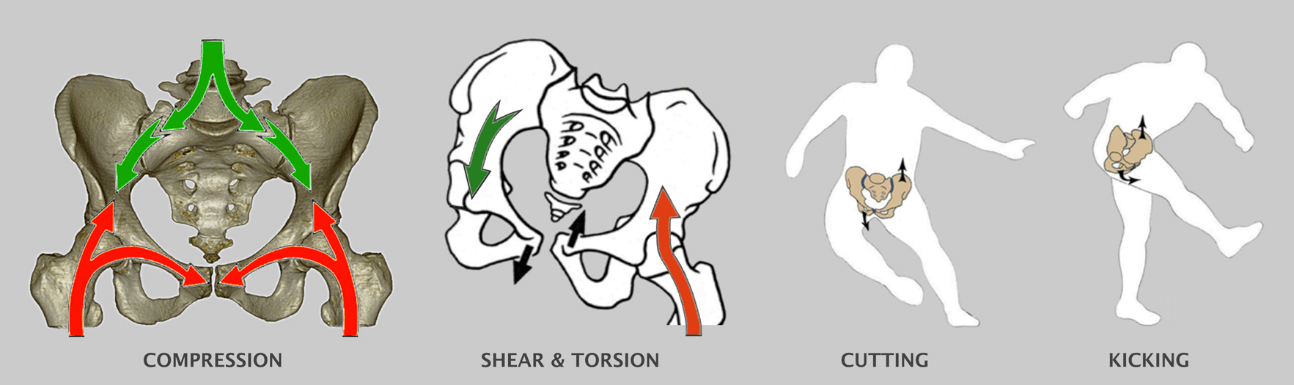
The most important intervention for this is management of abnormal pelvic mechanics and abnormal loads at an EARLY stage.
Relative rest (from running, cutting and kicking), combined with re-training of pelvic and core stabilisers (gentle neuromuscular exercises) can achieve full recovery.
Once the pubic bones have been stressed and there is significant bone bruising (previously called “Osteitis Pubis”), the pain can be very severe and begin to affect everyday activities. Running and kicking becomes completely inhibited by pain and this process resembles a stress fracture that takes anywhere from 3-6 months to recover from.
Prevention of Hip and Groin Pain
- If you are overweight, you may need to control your weight to avoid overstressing your hips
- Gradually increase the intensity of your workout, and ensure adequate rest and recovery between sessions
- Understand your hip morphology (shape) and accomodate to this to avoid physical activities that may worsen the pain
- Stretching the quadriceps and hamstring muscles, and maintain your gluteal strength and activity
- Wear proper fitting good quality running shoes with good shock absorption
Reference List
1. Tijssen M, van Cingel R, Willemsen L, de Visser E. Diagnostics of femoroacetabular impingement and labral pathology of the hip: a systematic review of the accuracy and validity of physical tests. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 2012 Jun;28(6):860–71.
2. Frank JM, Harris JD, Erickson BJ, Slikker W, Bush-Joseph CA, Salata MJ, et al. Prevalence of Femoroacetabular Impingement Imaging Findings in Asymptomatic Volunteers: A Systematic Review. Arthroscopy. 2015 Jun 1;31(6):1199–204.
3. Vahedi H, Aalirezaie A, Azboy I, Daryoush T, Shahi A, Parvizi J. Acetabular Labral Tears Are Common in Asymptomatic Contralateral Hips With Femoroacetabular Impingement. Clin Orthop. 2019 May;477(5):974–9.
4. Chan Y-S, Lien L-C, Hsu H-L, Wan Y-L, Lee MSS, Hsu K-Y, et al. Evaluating hip labral tears using magnetic resonance arthrography: a prospective study comparing hip arthroscopy and magnetic resonance arthrography diagnosis. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 2005 Oct;21(10):1250.
5. Khan W, Khan M, Alradwan H, Williams R, Simunovic N, Ayeni OR. Utility of Intra-articular Hip Injections for Femoroacetabular Impingement. Orthop J Sports Med [Internet]. 2015 Aug 31 [cited 2016 Mar 16];3(9). Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4622294/
6. Kemp JL, Beasley I. 2016 international consensus on femoroacetabular impingement syndrome: the Warwick Agreement—why does it matter? Br J Sports Med. 2016 Oct 1;50(19):1162–3.
7. Griffin DR, Dickenson EJ, O’Donnell J, Agricola R, Awan T, Beck M, et al. The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sports Med. 2016 Oct 1;50(19):1169–76.
8. Peters S, Laing A, Emerson C, Mutchler K, Joyce T, Thorborg K, et al. Surgical criteria for femoroacetabular impingement syndrome: a scoping review. Br J Sports Med. 2017 Nov 1;51(22):1605–10.
9. Philippon MJ, Schroder E Souza BG, Briggs KK. Hip arthroscopy for femoroacetabular impingement in patients aged 50 years or older. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 2012 Jan;28(1):59–65.
10. Kemp JL, Makdissi M, Schache AG, Pritchard MG, Pollard TCB, Crossley KM. Hip chondropathy at arthroscopy: prevalence and relationship to labral pathology, femoroacetabular impingement and patient-reported outcomes. Br J Sports Med. 2014 Jul 1;48(14):1102–7.